
Understanding PD-L1 as a Predictive Biomarker: Clinical Insights for Precision Oncology
PD-L1 expression has become a cornerstone in cancer immunotherapy decision-making. You rely on PD-L1 testing to predict which of your patients might benefit from immune checkpoint inhibitors. However, the biomarker’s clinical application involves complexities that require careful interpretation.
Key Takeaways
- PD-L1 testing guides immunotherapy decisions but shows variable predictive accuracy across cancer types and assays
- Five FDA-approved IHC assays measure PD-L1 differently, creating interpretation challenges at low-to-moderate expression levels
- Combining PD-L1 with TILs, TMB, or liquid biopsy markers improves patient selection beyond single-biomarker approaches
- Exosomal PD-L1 and AI-driven standardization address temporal heterogeneity and assay variability limitations
What is PD-L1 and Why Does It Matter in Your Practice?
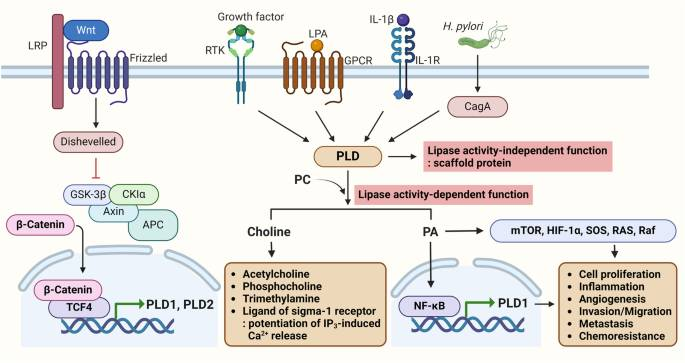
PD-L1 (Programmed Death-Ligand 1) is a protein expressed on tumor cells and immune cells. When PD-L1 binds to PD-1 receptors on T cells, it suppresses immune responses. Cancer cells exploit this pathway to evade immune surveillance.
Tumors upregulate PD-L1 to inhibit T-cell activity. Checkpoint inhibitors block this interaction, allowing the immune system to recognize and attack cancer cells. PD-L1 expression levels help you predict treatment response in your patients.
Higher PD-L1 expression often correlates with better outcomes from anti-PD-1/PD-L1 therapies. However, the correlation varies across cancer types. Not all patients with high PD-L1 respond, and some with low or negative PD-L1 still benefit.
How Does PD-L1 Testing Work in Clinical Settings?
Immunohistochemistry (IHC) remains the standard method for PD-L1 assessment. Pathologists analyze tumor biopsy samples using FDA-approved assays: 22C3, 28-8, SP142, SP263, and 73-10.
Each assay measures PD-L1 expression differently. Tumor Proportion Score (TPS) quantifies expression on tumor cells, while Combined Positive Score (CPS) includes both tumor and immune cells.
Common thresholds include 1%, 5%, and 50% positivity. A 50% cutoff typically indicates strong candidacy for monotherapy, while lower cutoffs may guide combination therapy decisions.
Head and neck cancers also require testing in many treatment algorithms. The specific assay you use depends on the planned therapeutic agent. Different drugs have companion diagnostics validated with specific assays.
At the recent ImmunoMark Summit in London, experts presented AI-driven approaches to PD-L1 standardization. These innovations aim to reduce interpretation variability across laboratories.
Does PD-L1 Expression Reliably Predict Patient Outcomes?
PD-L1 biomarker clinical validation has progressed through numerous trials. Over 80% of FDA approvals for checkpoint inhibitors involve PD-L1 as a correlate. Positive PD-L1 status predicts higher response rates in many cancers.
Studies show improved progression-free survival when PD-L1 expression is elevated. Overall survival benefits emerge in PD-L1-positive populations. Neoadjuvant settings demonstrate major pathological responses correlating with expression levels.
Combining PD-L1 with tumor-infiltrating lymphocytes (TILs) enhances prediction. The checkpoint inhibitor response biomarker performs better when contextualized with immune infiltration. TIL-rich, PD-L1-positive tumors show the strongest responses.
NCCN guidelines recommend PD-L1 testing to guide your therapy selection. Testing helps you identify patients likely to benefit from monotherapy versus combination approaches. Clinical decision-making balances efficacy predictions with safety considerations.
Higher PD-L1 may correlate with increased risk of severe adverse events. You must weigh response likelihood against toxicity potential. The biomarker informs but does not dictate your treatment decisions.
John Smeraglia from AstraZeneca delivered a keynote at ImmunoMark Summit London 2026 on biomarker strategy as a clinical decision-making tool. His presentation highlighted how integrating multiple biomarkers improves patient selection.
What Limitations Should Clinicians Recognize When Using PD-L1?
Understanding where PD-L1 testing falls short helps you make better-informed decisions. Several technical and biological factors can affect your interpretation of results.
- Assay variability creates interpretative challenges
Different assays produce discrepant results, particularly at low-to-moderate expression levels. Comparing results across platforms proves difficult without harmonization studies.
- Spatial and temporal heterogeneity limits biopsy accuracy
Single biopsies capture only one tumor region. PD-L1 expression varies across different metastatic sites and changes over time during treatment.
- Dynamic expression changes reduce predictive value
Treatment induces dynamic changes in PD-L1 expression. Your post-therapy biopsies may show different patterns than baseline samples captured weeks or months earlier.
- PD-L1-negative tumors can still respond
Non-inflamed tumor microenvironments without TILs challenge our reliance on PD-L1 alone. The biomarker misses responders in immunologically cold tumors.
- Primary resistance occurs despite high expression
Some of your patients with high PD-L1 experience primary resistance. Mechanisms beyond PD-1/PD-L1 drive immune evasion in these cases.
Tumor mutational burden (TMB), microsatellite instability, and other factors influence outcomes. A comprehensive panel discussion at the London 2026 edition of ImmunoMark Summit explored these resistance mechanisms. Experts from J&J and Roche shared insights on overcoming predictive limitations.
What Emerging Approaches Can Improve Predictions?
Exosomal PD-L1 offers a non-invasive alternative to tissue biopsy. Blood-based testing measures PD-L1 on extracellular vesicles. Liquid biopsies provide systemic tumor immune status information.
Exosomal PD-L1 shows promise for real-time monitoring of your patients. Serial measurements track treatment response dynamics. Accessibility surpasses tissue IHC, particularly for metastatic or hard-to-biopsy lesions.
Combined biomarker panels enhance your predictive accuracy. PD-L1 plus TMB identifies additional responders. Multi-omics approaches integrate genomic, transcriptomic, and proteomic data.
Circulating tumor cells (CTCs) add another dimension to our understanding. Digital pathology workflows improve reproducibility and standardization. Artificial intelligence models analyze complex biomarker patterns.
Sessions on extracellular vesicle profiling at ImmunoMark Summit demonstrated how liquid biopsy technologies complement traditional tissue testing. These approaches address temporal heterogeneity challenges.
Composite scores combining PD-L1 and TILs perform better than either alone. Integrated immune profiling captures microenvironment complexity. Multiplex immunofluorescence reveals spatial relationships between biomarkers.
How Are Regulatory and Commercial Landscapes Evolving?
Companion diagnostics require rigorous validation before approval. Regulatory bodies demand evidence of analytical and clinical validity. Multi-center studies establish performance characteristics across diverse populations.
Commercialization involves collaboration between diagnostic and pharmaceutical companies. Agilent recently received approvals for PD-L1 testing in ovarian cancer. Roche, Dako, and Ventana provide widely used platforms.
Laboratory implementation requires quality assurance programs in your institution. Proficiency testing ensures consistent interpretation. You and your pathology colleagues need training on scoring criteria specific to each assay.
Reimbursement policies influence testing adoption in your healthcare system. Insurance coverage varies by indication and region. Value-based care models emphasize biomarker-guided treatment selection.
Where Is Research Headed in PD-L1 Biomarker Development?
Ongoing research explores toxicity prediction using PD-L1 status. Understanding adverse event correlations improves your risk-benefit discussions with patients. Neoadjuvant trials investigate PD-L1 as a response predictor before surgery.
Novel immune checkpoint targets beyond PD-1/PD-L1 are emerging. LAG-3, TIM-3, and TIGIT represent next-generation targets. Combination strategies require new predictive biomarkers for your clinical toolkit.
Resistance mechanisms drive biomarker discovery efforts. Tumor microenvironment modulation affects PD-L1 expression. Metabolic influences on immune checkpoint pathways warrant investigation.
Epithelial-mesenchymal transition interacts with PD-L1 biology. Cancer cell intrinsic processes influence immunotherapy response. Comprehensive profiling moves beyond single biomarkers.
You can also join collaborative research initiatives that advance biomarker science. Multi-institutional studies generate the robust validation data that regulatory bodies require. Partnerships between academia and industry move discoveries from bench to bedside.
The Next-Gen Immuno-Oncology stream at ImmunoMark Summit London 2026 featured presentations on CAR-T multi-antigen targeting and ML-driven multispecific antibody engineering. These sessions explored how emerging therapies will require novel biomarker strategies. Get a quick overview of the summit in this short video.
Stay Current in This Rapidly Evolving Field With The ImmunoMark Summit
Scientific conferences let you exchange knowledge directly with peers working on similar challenges. Immuno-oncology biomarker events showcase data from recent trials and real-world studies. You can access specific implementation strategies used in other clinics and labs.
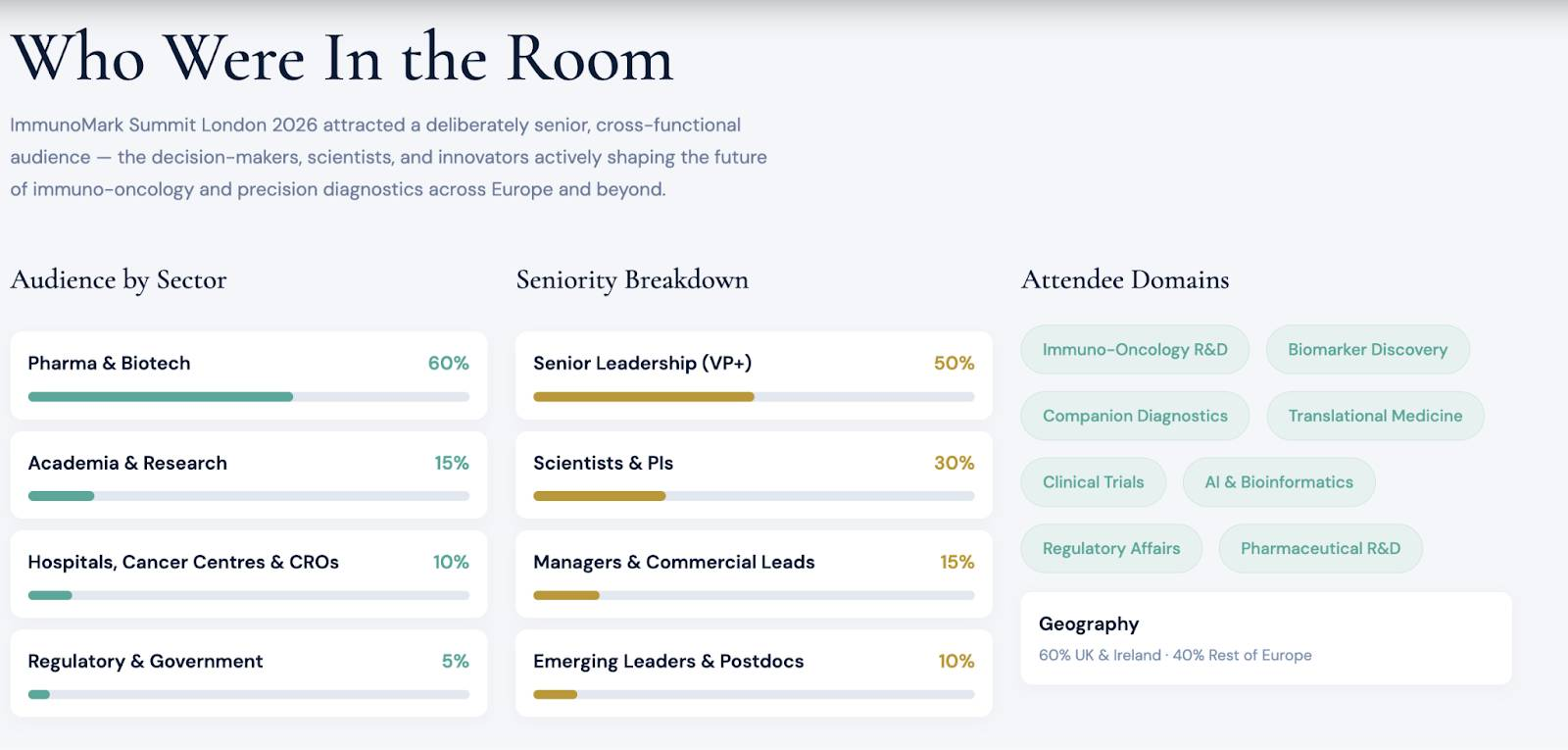
The ImmunoMark Summit 2026 UK Edition brought together 400+ senior professionals, with 50 expert speakers, in March 2026 at the DoubleTree by Hilton, Tower of London. Decision-makers from pharma, biotech, and academia attended two parallel streams over two days.
Caption: Attendees at the Immunomark 2026 edition
The Biomarkers & Companion Diagnostics stream covered home-sampling biomarkers and AI-driven PD-L1 standardization. Louis Boon from JJP Biologics keynoted on next-generation IO approaches. Half the attendees held senior leadership positions.
Yariv Hefez from Merck moderated a panel on biomarkers as market-makers in oncology. Panelists from J&J and Roche participated in the discussion. Post-event surveys showed nine out of ten attendees said they would recommend the summit to colleagues.
You can request the full event report by sharing your email ID below.
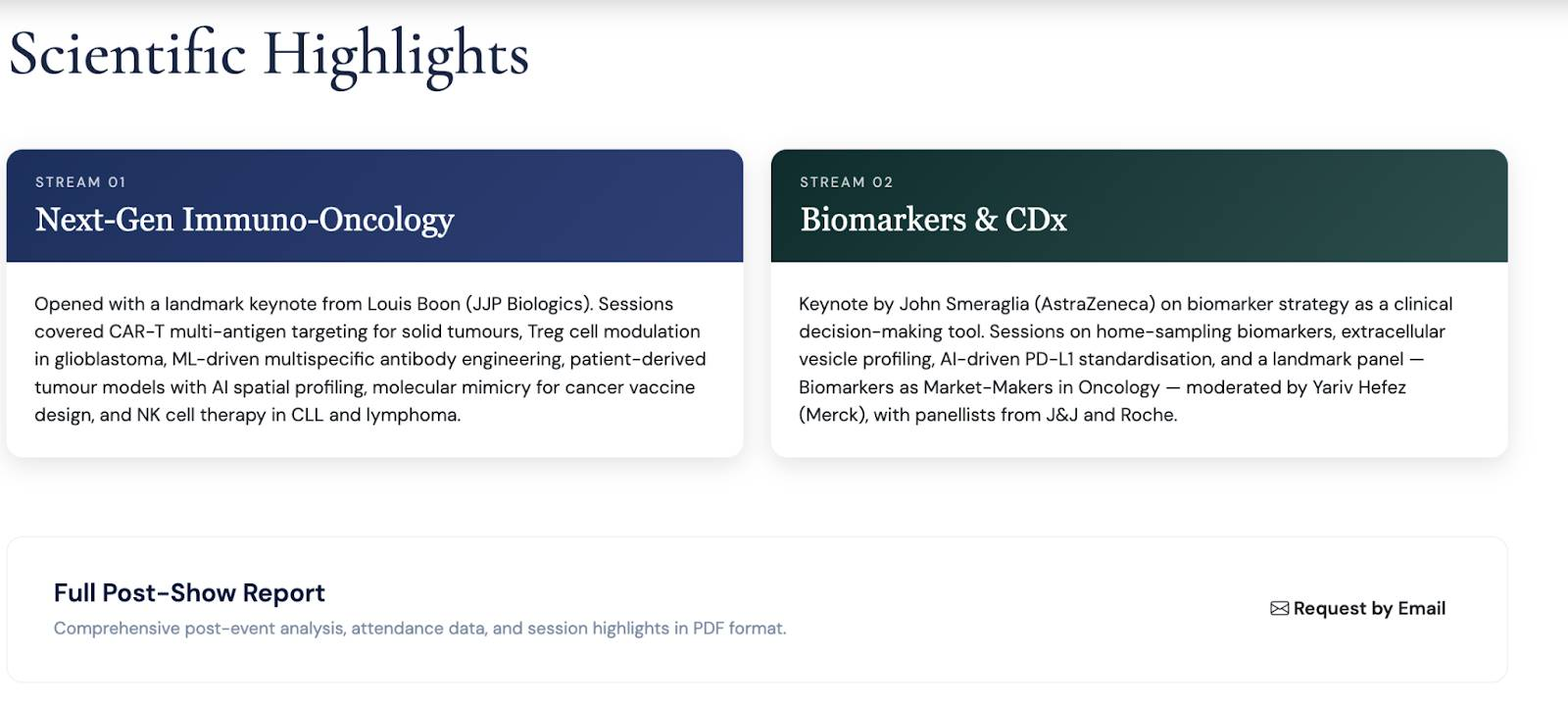
Get the post-show report here.
View highlights from ImmunoMark Summit London 2026 to see what innovations were discussed. The image gallery and post-show report showcase sessions on AI spatial profiling and molecular mimicry for cancer vaccine design.
We’re coming up with another edition in 2027. Register for ImmunoMark Summit Boston 2027 to connect with scientists and clinicians developing companion diagnostics. The upcoming edition runs dedicated tracks on companion diagnostics and next-gen IO biomarkers.
#Biomarkers
#CancerResearch
#ClinicalTrials
#IOConferences


